
The Skeleton Crew Guide to Bone Meds
May 21, 2026
Don’t Get Burned: Choosing Between Ice and Heat for Strains
May 28, 2026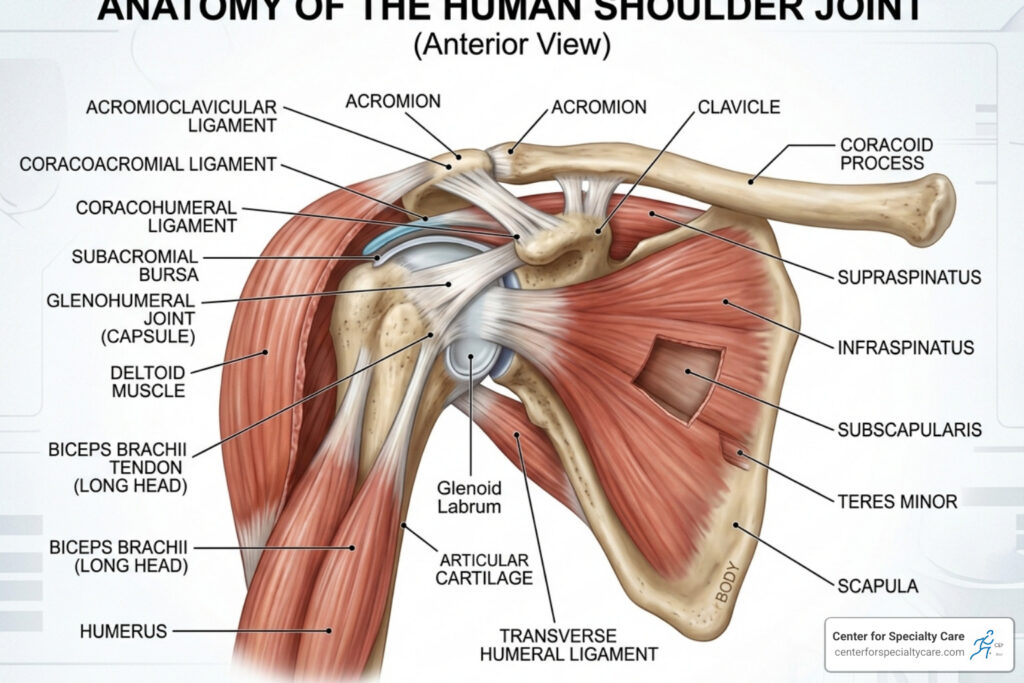
The Definitive Guide to Shoulder Joint Anatomy
The Most Mobile — and Most Vulnerable — Joint in Your Body
Shoulder joint anatomy is built around a remarkable trade-off: extraordinary range of motion in exchange for inherent instability. No other joint in the human body can move in as many directions, yet that same freedom makes it one of the most commonly injured areas people deal with.
Here is a quick overview of the key structures that make up the shoulder joint:
| Structure | Type | Primary Role |
|---|---|---|
| Humerus, scapula, clavicle | Bones | Form the bony framework |
| Glenohumeral joint | Ball-and-socket synovial joint | Enables wide range of arm movement |
| Acromioclavicular (AC) joint | Plane synovial joint | Connects clavicle to scapula |
| Rotator cuff (4 muscles) | Muscle group | Dynamic stability and rotation |
| Glenoid labrum | Fibrocartilage ring | Deepens the socket, resists dislocation |
| Glenohumeral ligaments | Ligaments | Passive restraints against dislocation |
| Subacromial bursa | Fluid-filled sac | Cushions tendons during movement |
The shoulder is actually made up of four separate articulations working together — the glenohumeral, acromioclavicular, sternoclavicular, and scapulothoracic joints. The glenohumeral joint is the main event: a large humeral head sitting in a shallow socket roughly four times smaller than the ball itself. Think of a golf ball balanced on a tee. That design allows you to lift, rotate, reach, and throw — but it also means soft tissues like the labrum, ligaments, and rotator cuff have to do a lot of heavy lifting to keep everything in place.
Understanding how these structures work together helps explain why shoulder pain happens — and what can be done about it.
I’m Dr. Corey Welchlin, a board-certified orthopedic surgeon with over 30 years of experience treating shoulder conditions including rotator cuff repairs and arthroscopic procedures, making shoulder joint anatomy a cornerstone of my daily clinical practice. That depth of hands-on experience shapes everything you’ll find in this guide.

The Skeletal Framework: Bones and Joints of the Shoulder
To understand how the shoulder works, we first have to look at the “chassis.” The shoulder isn’t just one single joint; it is a complex girdle that connects the upper limb to the axial skeleton. This connection is surprisingly minimal—the only bony attachment of the arm to the rest of the body is at the sternoclavicular joint, where your collarbone meets your breastbone.
The primary bones involved in shoulder joint anatomy include:
- Humerus: The upper arm bone. The rounded “head” of the humerus serves as the “ball.”
- Scapula: The shoulder blade. This flat, triangular bone sits on the back of the rib cage and contains the glenoid cavity (the socket).
- Clavicle: The collarbone. This acts as a strut, keeping the arm away from the thorax to allow for maximum range of motion.
These bones create several critical articulations. While we often focus on the ball-and-socket, the Acromioclavicular (AC) joint (where the clavicle meets the acromion of the scapula) and the Sternoclavicular (SC) joint are vital for transferring load and allowing the shoulder blade to move.
| Feature | Glenohumeral Joint | Acromioclavicular (AC) Joint |
|---|---|---|
| Type | Ball-and-Socket | Plane Synovial |
| Mobility | Extremely High | Low (Gliding) |
| Stability | Low (Relies on soft tissue) | High (Strong ligaments) |
| Primary Function | Arm rotation and reach | Scapular attachment and stability |
Understanding the Basics of Shoulder Joint Anatomy
The “star” of the show is the glenohumeral joint. Structurally, it is a multiaxial diarthrodial joint. The most striking feature of this joint is the disproportion between its surfaces. The glenoid fossa (the socket) is remarkably shallow. In fact, the surface area ratio of the humeral head to the glenoid is roughly 4:1. This means the socket only accommodates about one-third to one-fourth of the humeral head at any given time.
Furthermore, the glenoid cavity is typically retroverted by approximately 5° to 7°. This specific orientation, combined with the shallow depth, is why the shoulder is the most mobile joint in the body—and why it is often described as “insecure.” For a deeper dive into how these bones interact, you can explore more about Shoulder Joint: What It Is, Anatomy & How It Works.
The Scapulothoracic Articulation
While not a “true” anatomical joint in the sense of having a capsule and synovial fluid, the scapulothoracic articulation is a functional joint that is essential for shoulder health. It is the gliding movement of the scapula over the posterior thoracic cage (the ribs).
For every two degrees the humerus moves, the scapula must move one degree—a relationship known as scapulohumeral rhythm. If this rhythm is disrupted, you might experience “winging” of the shoulder blade or clicking sounds. We often see patients who complain of shoulder clicking and pain, which can sometimes be traced back to poor scapular mechanics or “snapping scapula syndrome.”
Soft Tissue Architecture: Muscles and the Rotator Cuff
If the bones provide the framework, the muscles provide the engine and the steering. Because the bony socket is so shallow, the shoulder relies heavily on “dynamic stabilizers”—muscles that actively contract to pull the humeral head into the center of the socket.
The shoulder is powered by several muscle groups:
- Deltoid: The large, triangular muscle that gives the shoulder its rounded shape. It is the primary mover for abduction (lifting the arm out to the side).
- Biceps Brachii: Specifically the long head of the biceps, which travels through the joint and helps stabilize the humeral head.
- Triceps: Plays a minor role in stabilizing the inferior (bottom) part of the joint.

A comprehensive look at Anatomy, Shoulder and Upper Limb, Shoulder shows that without these muscles, the arm would simply fall out of the socket. This is why shoulder treatment with physical therapy is so effective; by strengthening these muscles, we can compensate for ligamentous laxity or minor tears.
The Role of the Rotator Cuff in Shoulder Joint Anatomy
The rotator cuff is a group of four tendons and muscles that form a protective sleeve around the glenohumeral joint. Their primary job is to compress the humeral head into the glenoid fossa. The four muscles are:
- Supraspinatus: Initiates the first 15 degrees of abduction.
- Infraspinatus: Primarily responsible for external rotation.
- Teres Minor: Also assists in external rotation.
- Subscapularis: The largest and strongest, responsible for internal rotation.
When these muscles are healthy, they provide “dynamic stability.” However, because they live in a tight space under the acromion bone, they are prone to wear and tear. Many patients find that rotator cuff issues lead to a dull ache that worsens at night. If you are struggling with this, we have compiled expert tips for better sleep with rotator cuff pain.
Accessory Muscles and Tendons
Beyond the “Big Four,” other structures play a role in shoulder joint anatomy. The long head of the biceps tendon is unique because it is “intracapsular but extrasynovial”—it actually travels inside the joint capsule before attaching to the top of the glenoid.
We also look closely at the rotator cable, a thick band of fibers that acts like a suspension bridge, distributing forces across the rotator cuff tendons. As we age, the rotator cable often thickens to provide extra stability. Sometimes, pain in the shoulder isn’t actually in the joint itself but in the surrounding area, such as a muscle kink in the shoulder blade, which can be caused by the levator scapulae or rhomboid muscles.
Stability and Support: Ligaments and the Glenoid Labrum
Since the shoulder is so mobile, it needs a sophisticated “braking system” to prevent it from moving too far. This system consists of the joint capsule, ligaments, and a special ring of cartilage called the labrum.
The joint capsule itself is remarkably loose—twice the size of the humeral head—to allow for movement. However, it is reinforced by several thickened bands known as the glenohumeral ligaments. For a technical breakdown of these structures, the StatPearls guide on the glenohumeral joint is an excellent resource. When these ligaments become too loose, patients often experience shoulder joint pain and popping.
Primary Ligamentous Stabilizers
The ligaments act as “passive stabilizers.” They don’t contract like muscles; they simply become taut when the arm reaches the end of its range of motion.
- Superior Glenohumeral Ligament (SGHL): Prevents the humerus from sliding downward when the arm is at the side. (Absent in about 10% of people!)
- Middle Glenohumeral Ligament (MGHL): Provides stability when the arm is partially raised. (Absent in up to 30% of people!)
- Inferior Glenohumeral Ligament (IGHL): The most important stabilizer against anterior dislocation when the arm is raised and rotated outward.
- Coracoacromial Arch: Formed by the coracoid process, the acromion, and the coracoacromial ligament. This creates a “roof” over the humerus to prevent it from popping out upward.
If you feel your shoulder “shifting” or hear sounds during movement, check out our guide on why your shoulder might be popping.
The Glenoid Labrum and Supraglenoid Tubercle
The glenoid labrum is a ring of specialized fibrocartilage that lines the rim of the glenoid cavity. It serves two vital purposes:
- Deepening the Socket: It increases the depth of the glenoid by about 50%, allowing the “golf ball” to sit more securely on the “tee.”
- The Suction Effect: It creates a seal that maintains a negative pressure (a vacuum) inside the joint, which helps hold the bones together.
Injuries to the top part of the labrum, where the biceps tendon attaches, are called SLAP lesions (Superior Labrum Anterior to Posterior). These often cause clicking when raising the arm and are common in athletes who perform overhead throwing.
Clinical Relevance: Common Injuries and Anatomical Variants
Because of its complexity, the shoulder is prone to specific injury patterns. Statistics show that anterior dislocations account for 95% of all shoulder dislocations, usually occurring when the arm is forced into an abducted and externally rotated position.

When the humerus pops out of the socket, it often causes secondary damage:
- Bankart Lesion: A tear of the anterior-inferior labrum.
- Hill-Sachs Lesion: A compression fracture on the back of the humeral head caused by it hitting the edge of the glenoid.
These injuries are particularly common in high-impact events. If you’ve recently been in a collision, you might find our advice on shoulder pain after a car accident helpful for your recovery.
Anatomical Variants and Imaging Pitfalls
Not every shoulder looks the same on an MRI. There are several “normal” variations that can look like injuries to an untrained eye:
- Os Acromiale: A condition where the acromion bone fails to fuse, occurring in up to 15% of the population.
- Sublabral Foramen: A small hole under the labrum (found in 11% of people) that can be mistaken for a tear.
- Buford Complex: A rare variant (1.5–2%) where the anterior-superior labrum is missing, and the middle glenohumeral ligament is thickened.
Understanding these variants, as detailed in StatPearls – Glenohumeral Joint, is crucial for avoiding unnecessary surgery.
Neurovascular Supply and Movement Mechanics
The shoulder’s blood supply primarily comes from the anterior and posterior circumflex humeral arteries. Interestingly, the posterior artery provides about 64% of the blood to the humeral head.
The nerves are equally important. The axillary nerve wraps around the neck of the humerus and is at high risk during dislocations. The suprascapular nerve powers the supraspinatus and infraspinatus. If you are dealing with chronic pain that hasn’t responded to therapy, we sometimes discuss types of injections for shoulder pain to reduce inflammation around these nerves and tendons.

Frequently Asked Questions about Shoulder Anatomy
What are the four muscles of the rotator cuff?
The four muscles are the supraspinatus, infraspinatus, teres minor, and subscapularis. Together, they form a “cuff” that stabilizes the humerus and allows for rotation.
Why is the shoulder joint the most mobile in the body?
The shoulder’s mobility comes from its ball-and-socket design, a very shallow glenoid cavity (socket), and a loose joint capsule. This allows the arm to move in nearly every direction, including 360-degree circumduction.
What is the function of the glenoid labrum?
The labrum is a fibrocartilage ring that deepens the shallow shoulder socket and acts as a seal to create a suction effect, providing essential stability to the joint.
Conclusion
At the Center for Specialty Care, we believe that understanding your shoulder joint anatomy is the first step toward lasting relief. Whether you are dealing with a recent sports injury, a “kink” that won’t go away, or a complex rotator cuff tear, our team in Fairmont, St. James, and our Iowa locations is here to help.
We pride ourselves on 100% patient satisfaction and personalized care. We know that shoulder pain can stop you from enjoying life, which is why we offer both advanced surgical options and conservative non-surgical treatments. If you’ve been injured or are experiencing chronic pain, don’t wait—reach out to us today for a quick appointment and a clear path to recovery. For more tips on getting back to your normal routine after an injury, read our guide on recovering from shoulder pain after a car accident.



{kind=link}