
The Stubborn Shoulder Knot: More Than Just a Trigger Point
March 20, 2026
Everything you need to know about the Intracept procedure
March 24, 2026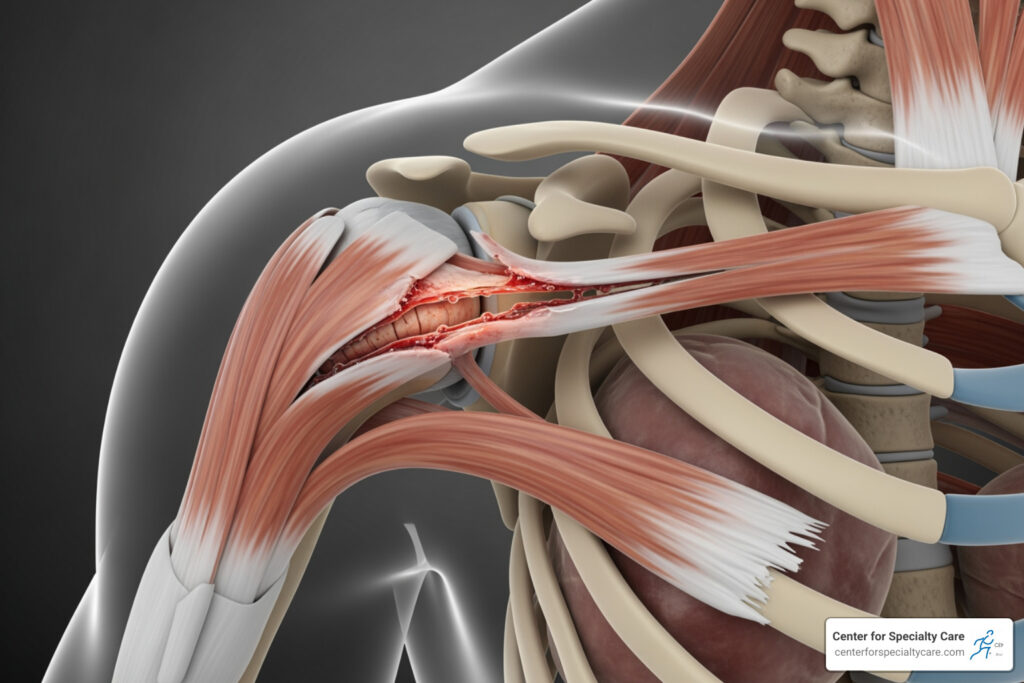
The Rotator Cuff Revealed: Anatomy, Injuries, and What a Tear Really Means
Why a Torn Rotator Cuff Deserves Your Attention
A torn rotator cuff is one of the most common causes of shoulder pain and weakness in adults — and it affects far more people than most realize.
Quick facts about a torn rotator cuff:
- It is a tear in one or more of the four tendons surrounding your shoulder joint
- Tears can be partial (the tendon is frayed but still attached) or full-thickness (a complete hole or detachment)
- About 30% of adults over 60 have one — and that rises to 62% by age 80
- The most commonly torn tendon is the supraspinatus
- About 8 out of 10 people with partial tears improve with nonsurgical treatment
Shoulder pain that flares up at night, weakness when lifting your arm overhead, or a clicking sensation during movement — these are signs your rotator cuff may be involved. Some people have a tear and feel nothing at all. Others find it limits nearly everything they do, from reaching a shelf to getting dressed in the morning.
The good news: a torn rotator cuff is treatable. Understanding what it is, what caused it, and what your options are is the first step toward getting better.
I’m Dr. Corey Welchlin, a board-certified orthopedic surgeon and sports medicine physician with over 30 years of experience treating torn rotator cuffs and other shoulder conditions at the Center for Specialty Care in Fairmont, Minnesota. In this guide, I’ll walk you through everything you need to know — from anatomy and diagnosis to treatment and recovery.
, types of tears (partial vs full-thickness), key symptoms (night pain, overhead weakness, clicking sounds), prevalence by age group (23% at 70, 51% at 80), and treatment pathways (nonsurgical vs surgical) with recovery timelines - torn rotator cuff infographic 4_facts_emoji_blue")
Basic torn rotator cuff vocab:
The Anatomy of Shoulder Stability
To understand why a torn rotator cuff is such a big deal, we first have to look at how the shoulder is built. The shoulder is a “ball-and-socket” joint, technically known as the glenohumeral joint. However, unlike the hip (where the ball sits deep in a socket), the shoulder socket is very shallow. Imagine a golf ball sitting on a tee, or a basketball on a dinner plate.
This design gives us an incredible range of motion—we can reach behind our backs, throw a baseball, and scratch our heads—but it makes the joint inherently unstable. That’s where the rotator cuff comes in. It is a group of four muscles and their tendons that wrap around the head of the humerus (the “ball”) and pull it firmly into the socket.
We often use the acronym SITS to remember these four muscles:
- Supraspinatus: This is the “workhorse” of the group. It sits on top of the shoulder and helps you lift your arm out to the side. Because it lives in a narrow space between bones, it is the most common site for a torn rotator cuff.
- Infraspinatus: Located on the back of the shoulder blade, this muscle allows you to rotate your arm outward (external rotation).
- Teres Minor: A small muscle that works alongside the infraspinatus to assist with external rotation.
- Subscapularis: The largest and strongest of the four, sitting on the front of the shoulder blade. It helps you rotate your arm inward (internal rotation), like when you reach for your back pocket.
When these muscles work together, they create a dynamic sleeve that keeps your shoulder centered. If one of these tendons is damaged, the “golf ball” can start to slide off the “tee,” leading to pain and mechanical issues. For a deeper dive into the structures of the arm, visit our page on shoulder anatomy.
What Defines a Torn Rotator Cuff?
Not all tears are created equal. When we talk about a torn rotator cuff, we are usually looking at two primary “flavors” of injury: acute and degenerative.
An acute tear happens suddenly. This is the classic “I felt a snap” moment. It usually occurs when you fall on an outstretched arm or try to lift something far too heavy with a jerking motion. In younger patients (under age 40), tears are almost always traumatic.
A degenerative tear, on the other hand, is a slow-motion injury. It’s the result of wear and tear over decades. As we age, the blood supply to these tendons naturally decreases, making it harder for the body to repair small micro-tears that occur during daily life. This is why the natural history of degenerative rotator cuff tears shows a massive spike in prevalence as we move from our 50s into our 80s.
| Feature | Acute Tear | Degenerative Tear |
|---|---|---|
| Onset | Sudden, traumatic event | Gradual, occurs over time |
| Pain Level | Intense, immediate pain | Dull ache that worsens slowly |
| Typical Patient | Athletes, workers, fall victims | Adults over age 40-50 |
| Common Cause | Falling, heavy lifting, accidents | Aging, repetitive stress, poor blood supply |
| Bilateral Risk | Usually one side | High chance of tear in the other shoulder |
Research indicates that an evidence-based approach to rotator cuff tears is essential because the treatment for a 25-year-old athlete with an acute tear is often very different from a 70-year-old with a chronic, wear-and-related tear.
Identifying a Partial Torn Rotator Cuff
A partial-thickness torn rotator cuff is often described as a “frayed rope.” The tendon is damaged, and some of the fibers have been pulled apart, but it is still attached to the bone.
Physicians often use the Ellman classification to grade these. Grade 1 is a small fray (less than 3mm), while Grade 3 involves more than 50% of the tendon’s thickness. While a partial tear might sound less serious, it can be incredibly painful because the remaining fibers are under increased stress. Interestingly, many people ask: will a torn rotator cuff heal on its own?. While the tendon rarely “knits” back together perfectly without surgery, the pain often resolves as the surrounding muscles get stronger.
Recognizing a Full-Thickness Torn Rotator Cuff
A full-thickness torn rotator cuff means the tendon has pulled all the way off the bone or has a complete hole through it. There is no longer a direct connection between the muscle and the arm bone.
When this happens, we look at the Codman classification, which measures the size of the hole—from “small” (under 1cm) to “massive” (over 5cm or involving multiple tendons). Over time, if a full-thickness tear isn’t addressed, the muscle can begin to shrink (atrophy) and the tendon can pull back away from the joint (retraction). This makes the management of full-thickness rotator cuff tears more complex, as retracted muscles are much harder to repair successfully.
Symptoms, Risks, and the Impact of Aging
The “hallmark” symptom of a torn rotator cuff is pain at night. Many of our patients in Fairmont and Estherville tell us they can’t sleep on the affected side, or that a deep, dull ache wakes them up the moment they roll over.
Other common symptoms include:
- Overhead Weakness: Struggling to reach into a high cabinet or brush your hair.
- Clicking or Popping: A “crunchy” sensation (crepitus) when moving the arm.
- Pain in the Deltoid: While the tear is in the cuff, the pain often radiates down the side of the arm.
- Limited Range of Motion: Stiffness that makes it hard to reach behind your back.
The Age Factor Aging is the single biggest risk factor for a torn rotator cuff. Scientific research on age-related prevalence shows that by age 80, a majority of adults have some form of a tear, even if they don’t have symptoms. Other risks include smoking (which further reduces blood flow to tendons), obesity, and occupations that require repetitive overhead work, such as painting or carpentry.
If your shoulder pain is interfering with your daily life, it might be time to see a doctor for shoulder problems to get a clear diagnosis.
Diagnosis and Treatment Pathways

When you visit us at the Center for Specialty Care, we don’t just rely on fancy machines; we start with a conversation and a physical exam. We use specific “special tests” to isolate each muscle:
- Jobe Test (Empty Can): We ask you to hold your arms out like you’re emptying a soda can while we apply downward pressure. This tests the supraspinatus.
- Drop Arm Test: We raise your arm out to the side and ask you to lower it slowly. If the arm “drops” suddenly, it often indicates a significant torn rotator cuff.
- Bear Hug Test: This checks the subscapularis on the front of the shoulder.
While X-rays are great for looking at bone spurs or arthritis, they don’t show tendons. To see the tear itself, an MRI is the gold standard. It allows us to see the size, location, and “age” of the tear. For more on how we navigate these findings, check the diagnosis and management of rotator cuff pathology.
Nonsurgical Management and Physical Therapy
Believe it or not, surgery isn’t always the first answer. About 80% of people with partial tears get better without ever stepping into an operating room. Our goal is to settle the inflammation and then strengthen the “backup” muscles to take the load off the torn tendon.
Nonsurgical options include:
- Activity Modification: Avoiding the specific overhead movements that hurt.
- NSAIDs: Medications like ibuprofen to reduce swelling.
- Steroid Injections: A “reset button” for inflammation. You can learn more about the types of injections for shoulder pain relief.
- Physical Therapy: This is the cornerstone of recovery. A skilled therapist can help you regain motion and strength. We offer many physical therapy tips for fast recovery to help our patients stay on track.
Surgical Interventions for Severe Tears
If nonsurgical treatments fail after 6 to 12 months, or if you have a large, acute tear that causes significant weakness, surgery may be the best path forward.
Most modern rotator cuff repairs are done via arthroscopy. We use tiny incisions and a camera (arthroscope) to reattach the tendon to the bone using small anchors. In cases of “massive” or “irreparable” tears in older patients with arthritis, we might discuss a reverse shoulder replacement, which changes the mechanics of the shoulder so the deltoid muscle can do the work of the missing rotator cuff. You can find more info about shoulder surgery on our dedicated service page.
Recovery Expectations and Long-Term Outlook
Recovery from a torn rotator cuff is a marathon, not a sprint. Whether you choose surgery or physical therapy, patience is required.
The Post-Surgery Timeline:
- Weeks 0-6: You’ll likely be in a sling to protect the repair. This is the “passive” phase where we move the arm for you, but you don’t use your own muscles.
- Months 2-4: We begin active motion and light strengthening.
- Months 4-6: You start regaining real-world strength and function.
- 1 Year+: Full recovery and return to heavy lifting or sports.
Scientific research on treatment outcomes suggests that both surgical and nonsurgical groups show the most significant improvement around the 12-month mark. The long-term prognosis is generally excellent, provided you stick to your rehab and maintain good posture and shoulder mechanics.
Frequently Asked Questions about Rotator Cuff Tears
How do I know if my rotator cuff is torn or just strained?
A strain (tendinitis) usually involves inflammation without a physical break in the tissue. It often improves quickly with rest and ice. A torn rotator cuff usually involves persistent weakness—if you literally cannot lift your arm, or it feels like it “gives out,” a tear is much more likely.
Can a rotator cuff tear heal without surgery?
A full-thickness tear will not physically “knit” back together on its own because the muscles are constantly pulling the edges apart. However, you can “functionally” heal. By strengthening the other muscles in the shoulder, many people can live pain-free lives with a tear.
Why does my shoulder pain get worse at night?
When you lie down, the effects of gravity change, and the humerus can shift slightly in the socket, putting pressure on the torn tendon. Additionally, the lack of daytime distractions makes you more aware of the dull, throbbing ache that characterizes cuff injuries.
Conclusion
A torn rotator cuff can feel like a major roadblock, but it doesn’t have to be the end of your active lifestyle. Whether you’re dealing with a recent sports injury or the cumulative effects of a lifetime of hard work, there is a clear path to relief.
At the Center for Specialty Care, we take pride in offering personalized, high-quality orthopedic care to our neighbors in Fairmont, MN, Estherville, IA, and the surrounding communities. Our goal is 100% patient satisfaction, and we achieve that by listening to your goals—whether that’s returning to the golf course or simply being able to sleep through the night without pain.
If you’re tired of living with shoulder pain, don’t wait for it to get worse. Early intervention often leads to better results and can prevent a small tear from becoming a massive one. Schedule a consultation for shoulder pain with us today, and let’s get you back to moving without limits.



{kind=link}
{kind=link}