
Knot Today! Banishing Those Pesky Shoulder Blade Knots for Good
March 31, 2026
Navigating your Intracept procedure recovery journey
April 2, 2026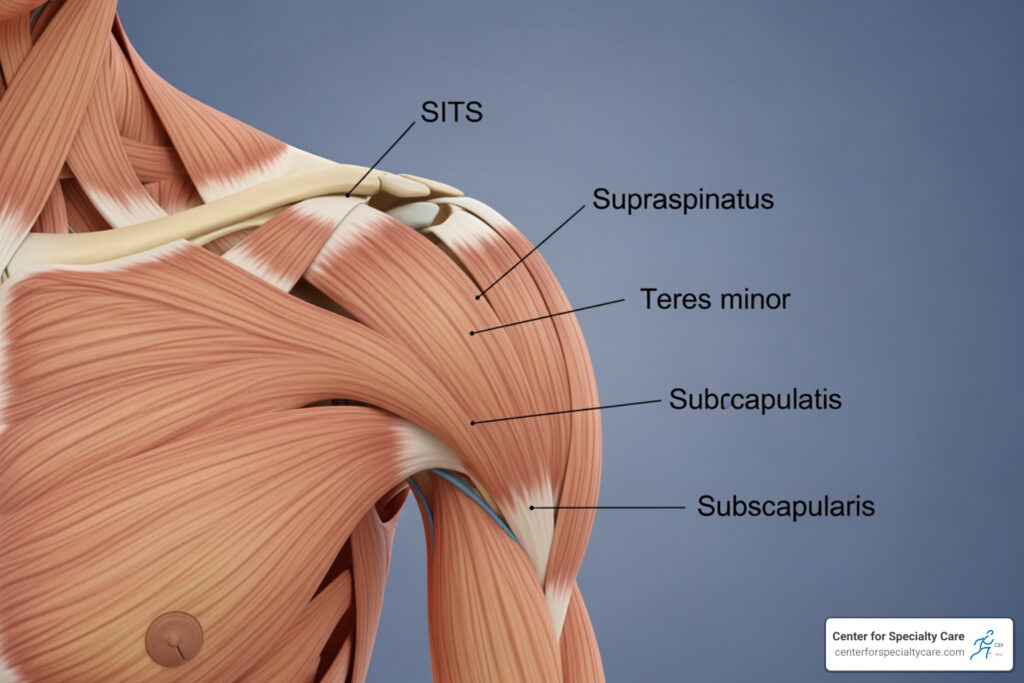
A Deep Dive into Rotator Cuff Muscles and Tendons
What Is Rotator Cuff Anatomy? A Quick Overview
Rotator cuff anatomy refers to the group of four muscles and their tendons that wrap around the shoulder joint, holding the upper arm bone firmly in place while allowing a wide range of motion.
Here’s a quick snapshot of the four muscles — often remembered by the acronym SITS:
| Muscle | Location | Primary Role |
|---|---|---|
| Supraspinatus | Top of shoulder blade | Initiates arm abduction (lifting) |
| Infraspinatus | Back of shoulder blade | External rotation |
| Teres Minor | Lower back of shoulder blade | External rotation and stability |
| Subscapularis | Front of shoulder blade | Internal rotation |
Together, these muscles form a cuff of tissue around the glenohumeral joint — the ball-and-socket joint that gives your shoulder its remarkable range of motion. Think of it like a golf ball sitting on a sideways tee: the socket is shallow, so the rotator cuff muscles do the heavy lifting to keep everything in place.
This structure is incredibly capable — but also vulnerable. When any part of it breaks down, the result can be pain, weakness, and lost function that affects everyday life.
I’m Dr. Corey Welchlin, a board-certified orthopedic surgeon with over 30 years of experience treating shoulder conditions — including rotator cuff anatomy problems ranging from tendonitis to complex surgical repairs. Understanding the structure of the rotator cuff is the foundation of everything I do for patients at the Center for Specialty Care, and I hope this guide gives you the clarity you need.

Rotator cuff anatomy terms to know:
The Four Muscles of Rotator Cuff Anatomy
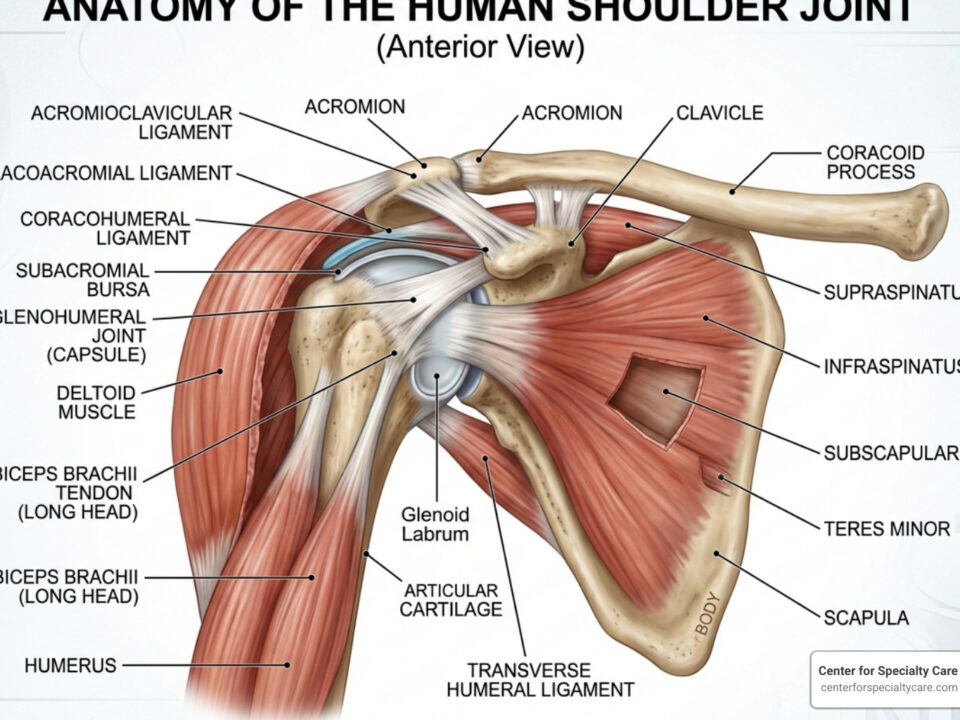
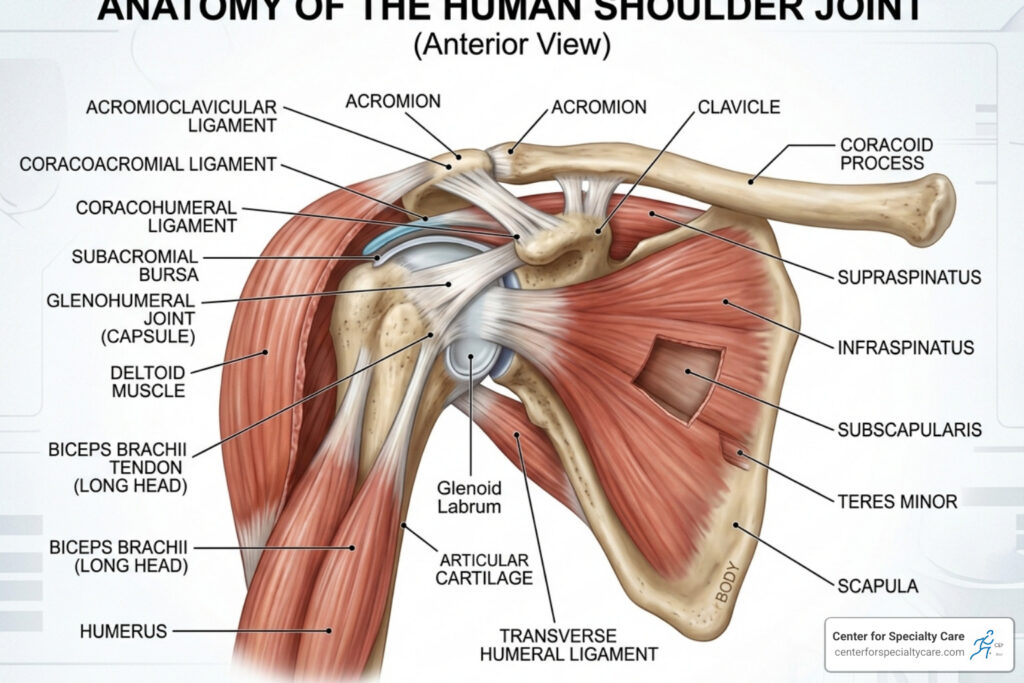
When we talk about the rotator cuff anatomy, we are describing a sophisticated “musculotendinous collar.” This collar is formed by the blending of four distinct muscle-tendon units that originate on the scapula (shoulder blade) and attach to the humerus (upper arm bone). These muscles don’t just sit next to each other; their tendons actually interweave with the joint capsule to create a continuous protective sleeve around the joint.

1. Supraspinatus
The supraspinatus is the most well-known of the group, primarily because it is the most commonly injured. It sits in the supraspinatus fossa—a horizontal groove at the very top of your shoulder blade. Its tendon passes underneath the acromion (the “roof” of your shoulder) to attach to the top of the humerus. Because it lives in such a tight space, it is highly susceptible to “impingement” or pinching.
2. Infraspinatus
Located just below the spine of the scapula, the infraspinatus covers most of the back of the shoulder blade. It is a thick, triangular muscle that provides significant power for external rotation. Recent research suggests that the infraspinatus actually occupies a larger portion of the attachment site on the humerus than we previously thought, making it a heavy hitter for shoulder stability.
3. Teres Minor
This is a narrow, elongated muscle that sits just below the infraspinatus. While smaller than its neighbors, it works in tandem with the infraspinatus to rotate the arm outward. Interestingly, in about 50% of people, the teres minor has its own distinct fascial compartment, which helps it function independently.
4. Subscapularis
The subscapularis is the “odd one out” because it is the only rotator cuff muscle located on the front (anterior) side of the shoulder blade. It is the largest and strongest of the four. It fills the entire subscapular fossa—the part of the shoulder blade that rests against your ribs. It is the primary internal rotator of the arm and is crucial for activities like reaching behind your back or tucking in a shirt.
For a deeper technical look at these structures, you can explore the Anatomy of the Rotator Cuff through the NIH StatPearls database.
Origins and Insertions in Rotator Cuff Anatomy
To understand why the shoulder moves the way it does, we have to look at where these muscles start and end. In medical terms, we call these “origins” and “insertions.”
- The Origins: All four muscles start on the scapula. They occupy specific “fossae” or shallow depressions on the bone that provide a wide surface area for the muscle fibers to grip.
- The Insertions (The Footprint): This is where the magic happens. The tendons attach to two bumps on the head of the humerus: the greater tuberosity and the lesser tuberosity.
- The Supraspinatus, Infraspinatus, and Teres Minor all attach to the greater tuberosity on the top and back.
- The Subscapularis attaches to the lesser tuberosity on the front.
The area where the tendon grips the bone is called the “footprint.” For example, the supraspinatus footprint is roughly triangular, measuring about 12.6 mm from front to back. Understanding these precise dimensions is vital for us during surgery; if we are repairing a tear, we want to reattach the tendon to its original footprint as accurately as possible to restore strength.
The health of these attachment points depends heavily on blood flow. You can read more about the vascular pathways in this study on the Arterial Supply to the Rotator Cuff Muscles.
Primary Functions and Movement Mechanics
The rotator cuff anatomy serves two main purposes: moving the arm and keeping the joint stable.
- Abduction Initiation: While the large deltoid muscle does the heavy lifting to move your arm away from your body, the supraspinatus is responsible for the first 0 to 15 degrees of that motion. Without it, the deltoid would simply pull the arm bone upward into the “roof” of the shoulder instead of swinging it out.
- Rotation: The infraspinatus and teres minor rotate the arm outward (external rotation), while the subscapularis rotates it inward (internal rotation).
- Dynamic Stabilization: This is the most critical role. As you move your arm, these four muscles pull the “ball” of the humerus tightly into the “socket” of the glenoid. We call this “concavity compression.”
If you’ve noticed your shoulder making strange noises while performing these movements, you might find our guide on shoulder joint pain and popping relief helpful.
Shoulder Stability and the Glenohumeral Joint
The shoulder is the most mobile joint in the human body, but that mobility comes at a price: instability. Unlike the hip joint, which is a deep “ball and socket,” the shoulder joint is shallow.
To compensate for this shallow socket, the body uses several stabilizers:
- The Labrum: A ring of specialized cartilage that deepens the socket.
- The Capsule and Ligaments: These provide “static” stability (they don’t move).
- The Rotator Cuff: These provide “dynamic” stability. They are the active guardians of the joint.
When the rotator cuff muscles contract, they compress the humeral head into the glenoid. This creates a suction-like effect that prevents the ball from sliding out of the socket. If the rotator cuff is weak or torn, the ball can shift upward or forward, leading to pain and further injury.
| Stabilizer Type | Component | Role |
|---|---|---|
| Static | Glenoid Labrum | Deepens the socket by 50% |
| Static | Glenohumeral Ligaments | Prevents extreme shifts |
| Dynamic | Rotator Cuff Muscles | Centers the ball in the socket |
| Dynamic | Long Head of Biceps | Assists in centering the ball |
We specialize in restoring this delicate balance. You can learn more about our shoulder services and how we address instability.
Blood Supply, Innervation, and the Coracoacromial Arch
The “machinery” of the rotator cuff requires a steady supply of nutrients and clear electrical signals from the brain to function.
Innervation (The Nerves)
The muscles are powered by branches of the brachial plexus:
- Suprascapular Nerve: Powers the supraspinatus and infraspinatus. It passes through a narrow notch in the shoulder blade, where it can sometimes become compressed by cysts.
- Axillary Nerve: Powers the teres minor (and the deltoid).
- Upper and Lower Subscapular Nerves: Power the subscapularis.
Blood Supply
The tendons of the rotator cuff, particularly the supraspinatus, are known for having a “critical zone” near their attachment point where blood supply is naturally thinner. This area becomes even more “blood-starved” as we age, which is one reason why degenerative tears are so common in patients over 40. The primary vessels involved are the suprascapular artery, the subscapular artery, and the posterior circumflex humeral artery.
The Coracoacromial Arch
Above the rotator cuff lies a “roof” made of bone (the acromion) and a ligament (the coracoacromial ligament). This space is called the subacromial space. Inside this space sits the subacromial bursa, a fluid-filled sac that acts as a lubricant. If the acromion is hooked or tilted (morphology), or if the bursa becomes inflamed (bursitis), it can rub against the rotator cuff tendons, leading to impingement syndrome.
Common Pathologies and Risk Factors
Because the rotator cuff anatomy is so complex and sits in such a tight space, several things can go wrong. We often view these issues as a “continuum”—it starts with minor irritation and can progress to a massive tear.
- Tendonitis and Bursitis: This is inflammation caused by repetitive overhead use. It’s common in painters, carpenters, and athletes.
- Partial-Thickness Tears: The tendon is damaged but not completely severed. A specific type called a PASTA lesion (Partial Articular Supraspinatus Tendon Avulsion) is a common injury we see in active patients.
- Full-Thickness Tears: The tendon is completely detached from the bone. These can be “acute” (from a fall or heavy lift) or “degenerative” (wearing out over time).
Key Statistics on Rotator Cuff Health
- Age: By age 70, over 70% of people have some form of rotator cuff tear, though many have no symptoms.
- Opposite Shoulder Risk: If you are over 66 and have a tear in one shoulder, there is a 50% chance you have one in the other shoulder—even if it doesn’t hurt yet!
- Trauma: If you are over 40 and dislocate your shoulder, there is a 50% chance you also tore your rotator cuff during the injury. By age 70, that chance jumps to 100%.
- Genetics: Siblings of people with tears are twice as likely to have a tear themselves.
Many patients ask, “Will a torn rotator cuff heal on its own?” The short answer is that while the pain may go away with therapy, the physical tear in the tendon does not knit back together without surgical intervention.
Clinical Diagnosis of Rotator Cuff Anatomy Issues
When you visit us at the Center for Specialty Care, we use a combination of physical tests and high-tech imaging to see exactly what’s happening inside your shoulder.
- Physical Exam: We use “cluster tests” to isolate each muscle. For example, the Jobe’s Test (or Empty Can Test) checks the supraspinatus, while the Hawkins-Kennedy Test looks for impingement.
- MRI: This is the “gold standard.” It allows us to see the size of a tear, how far the tendon has retracted, and whether the muscle has begun to turn into fat (fatty atrophy).
- Ultrasound: This is a great, cost-effective tool that allows us to look at the shoulder while it is in motion.
Early diagnosis is key to a faster recovery. Check out our shoulder treatment and physical therapy tips for more on the diagnostic process.
Treatment Options and Surgical Recovery
Our goal is always to start with the least invasive option that will get you back to the activities you love.
Non-Surgical Management
For tendonitis or small partial tears, we often recommend:
- Rest and Activity Modification: Avoiding overhead reaching for a period.
- Physical Therapy: Strengthening the surrounding muscles to take the pressure off the cuff.
- Corticosteroid Injections: To reduce inflammation and provide a “window of relief” so you can participate in therapy.
Surgical Repair
If conservative care doesn’t work, or if the tear is acute and large, surgery may be necessary. Most repairs today are done arthroscopically—using tiny cameras and instruments. We use “suture anchors” (tiny screws that eventually dissolve or stay permanently in the bone) to stitch the tendon back onto its original footprint.
Recovery Timeline
- Weeks 0-6: You’ll likely be in a sling to protect the repair.
- Weeks 2-6: Passive physical therapy begins (the therapist moves the arm for you).
- Months 3-6: Active strengthening begins.
- Month 6+: Return to full activities, including sports.
One of the biggest hurdles during recovery is sleep. We’ve put together some expert tips on how to relieve rotator cuff pain at night to help you get the rest you need.
Frequently Asked Questions about Rotator Cuff Injuries
Will small rotator cuff tears heal themselves?
No, rotator cuff tears do not have the ability to heal themselves because the tendons have a limited blood supply and are under constant tension. However, many tears can become asymptomatic. This means that through physical therapy and activity changes, the shoulder can function well and remain pain-free even if the tear is still physically present.
Are rotator cuff tears and frozen shoulder related?
They are separate conditions, but they can happen at the same time. Frozen shoulder (adhesive capsulitis) involves the joint capsule becoming thick and scarred, while a rotator cuff tear involves the tendons. Sometimes, the pain from a tear causes a patient to stop moving their arm, which then leads to the shoulder “freezing” up.
What are the chances of surgically repairing an old minor tear?
The chances are generally very good! As long as the muscle is still healthy and hasn’t been replaced by fat (atrophy), and the tendon hasn’t retracted too far away from the bone, we can usually perform a successful repair. Even if a tear happened a long time ago and you only tried physical therapy, surgery remains a viable option if your symptoms persist.
Conclusion
The rotator cuff anatomy is a masterpiece of biological engineering, providing the stability and power needed for everything from throwing a baseball to reaching for a coffee mug. However, because it operates in such a crowded space and handles so much stress, it requires careful attention when pain arises.
At the Center for Specialty Care, we are committed to providing personalized orthopedic care. Whether you are in Fairmont, MN, or our locations in Iowa, we offer quick appointment availability and a comprehensive range of surgical and non-surgical treatments. We believe in 100% patient satisfaction and will work with you to create a recovery plan tailored to your life.
If you’re struggling with shoulder pain, don’t wait for a small problem to become a major tear. Schedule a consultation for shoulder pain today and let’s get you back to moving without limits.


{kind=link}
{kind=link}
{kind=link}